Inomed Stockert Neuro N50. A versatile
RF lesion generator and stimulator for
countless applications and many uses
Multigen RF lesion generator .
INTRAOPERATIVE MRI RESULTS DURING THE PERIOD
2013-2018 IN NEUROSURGERY AND SPINE SURGERY.
Author: Munir Elias.
M.D, Ph.D.
Abstract Background:
High-field intraoperative MRI is gaining increasing recognition as
an invaluable tool in neurosurgery and spine surgery where the
questions and problems concerning morphologic data arising during the surgery need quick
answers. We report the initial experience of a dedicated 3-T
intraoperative MRI unit with all MRI
neuro applications, neurophysiologic monitoring, MRI compatible
anesthesia machine with MRI compatible monitoring vital devices and
specially constructed sliding door and second dockable table in the
management of certain neurosurgical and spine surgery.
Methods:
Well documented twenty seven patients, among many not mentioned (mean age 44 years; range 3–85
years) underwent IoMRI between November 2013 and April 2018, Using a 3-T MR scanner located adjacent to
the neurosurgical operating theater that is equipped with
neurophysiologic facilities. IoMRI was performed either to assess the
extent of tumor resection after surgical impression of
complete/intended tumor resection or to update the next steps in
surgery. The
surgical aims, IoMRI findings, extent of tumor resection,
escalations of possible events in the surround or remotely and
follow-up data were reviewed. Concerning functional data, ISIS
Neuroexplorer 32 channel with all needed protocols is helpful in
detecting the functionality of the neural structures during surgery.
Results:
Complete resection of tumors was intended in certain tumors without
proper borders in 15 operations. IoMRI confirmed complete resection
in 30% of this group. IoMRI findings led to
further resection in this last group. In 3 of 15 (20%), IoMRI was equivocal
for residual tumor and when there was evidence of residual tumor was found on
re-inspection, further IoMRI was repeated until the situation was
considered acceptable, or further radical resection will harm the
patient outcome. Some patients required follow up MRI even the same
day of operation or the 2-3 postoperative days.
Conclusions:
IoMRI has led to increased rate of tumor
resection and a change in surgical strategy with further tumor
resection in 70% of patients. While interpreting IoMRI, it is
important to be aware of the known pitfalls. Using the MRI neuro
software is more important than performing the standard protocol.
New problems and new findings took place during the use of these
technologies which needs future solutions.
Keywords: Magnetic resonance imaging, intraoperative MRI,
intraoperative neurophysiologic monitoring, neurosurgery, spine
surgery
INTRODUCTION
Neurosurgery and spine surgery have a lot of challenges. During
surgery, even with an experienced neurosurgeon, safe and real time answers must be ready by
using intraoperative MRI and neurophysiologic
monitoring. Brain tumors are a major cause of mortality and
long-term morbidity. Surgery is a vital part of management, and the
degree of primary surgical resection is a major prognostic factor in
several tumor types, including the more common malignant tumors such
as medulloblastoma, high-grade glioma, and ependymoma.[1,8,10] For
low-grade glioma, the most common brain tumor in childhood,
glioblastoma multiforme, high grade astrocytomas, and many other
conditions in adults, complete surgical excision is generally
provide more acceptable results.
High-field intraoperative MRI (IoMRI) is rapidly developing as an
aid to safe and effective neurosurgery and spine surgery. The use of neurophysiologic
monitoring and operating microscopes is well established in aiding
tumor resection. Whilst the role of IoMRI is well documented in
adult neurooncology practice, there is tendency to accept this setup
as standard in all fields of neurosurgery and spine surgery.
HIGH-FIELD IOMRI FACILITY: DESIGN AND SAFETY CONSIDERATIONS
The IoMRI system at Al-Shmaisani hospital, Amman-Jordan, involves a two-room
solution which allows independent function of individual components.
It is equipped with a 3 tesla Siemens Skyra with a length of 157 cm
and an inner bore of 70 cm, 2 dockable tables, TxRx head coil 3T,
all needed coils, all neurosuite more than 30 software, such as
fibertraking, spectroscopy, TWIST, SWI, functional MRI, ASL and many
unmentioned here software.
The facility design allows for diagnostic MRI when not needed for
IoMRI, making the facility economically viable and allowing for
optimal use of this expensive technology. The IoMRI suite is located
next to the neurosurgical operating theater, separated by special
sliding door produced by Siemens to prevent bacterial and
ferromagnetic interference. This arrangement enables independent use
of the neurosurgical operating theater and the MRI scanner when
IoMRI is not needed.
Special coils and hardware are necessary to facilitate maintenance
of sterility of the operative field. IoMRI can be performed using a
dedicated Inomed Riechert-Mundinger system with ceramic ring and
carbonized screws. In most cases, the wound was temporarily closed,
sent to the scanner and connected to the other MRI compatible
anesthesia machine. Safe transfer of the patient into the MRI scanner
is achieved by the same dockable table. The other second dockable
table is intended for security measures in case of troubleshooting
of the first. If the patient is under G.A., then the endotrachial
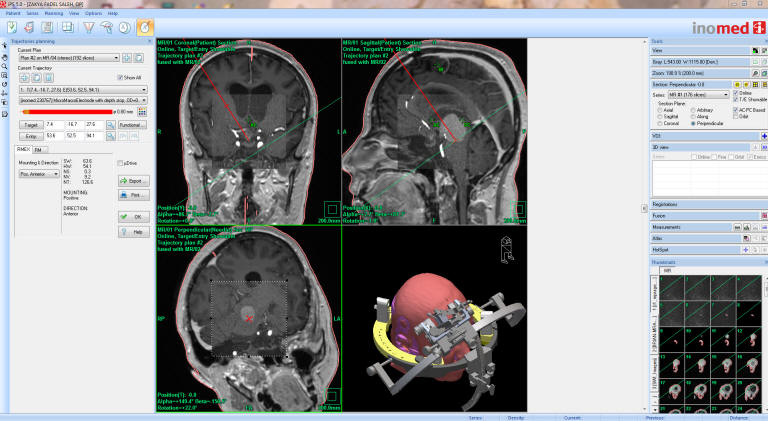
tube must be MRI compatible. The iPs 5 Inomed software is an
excellent program to facilitate certain tracks, avoiding during that
the arteries, veins and important structures.
IoMRI poses certain challenges in terms of safe use, both for the
theater staff and for the anesthetized patient. The general safety
and anesthetic considerations for IoMRI are outlined in many
articles. For more information, please click
here!12
MATERIALS AND METHODS Patients
Between November 2013 and March 2018, IoMRI was performed on many
patients. The fully illustrated documented cases taken to the study
were 27 cases with mean age was 44
years (range 3-85 years).
Imaging
IoMRI was performed on a Skyra 3-T scanner, with all neuro MRI
software, located alongside the neurosurgical operation theater and
equipped with neuronavigation facility and intraoperative
neuromonitoring using ISIS 32 channels with complete setup from
Inomed. Preoperative imaging was performed on the 3-T scanner.
The surgical aim (complete, subtotal, near-total resection) was
defined preoperatively by a multidisciplinary team.
The intraoperative imaging sequences were tailored to tumor
characteristics and surgical aims. IoMRI sequences
performed with all necessary neuro protocols, related to the case
and situation. In complex
operations, more than one intraoperative scan may be required. The
specific parameters for the MR sequences have been described by
Abernethy et al.[2] High-field IoMRI also allows for advanced
multimodal imaging to be performed, which can aid in
surgical decision making.
IoMRI was limited to the precontrast sequences if there was
unequivocal evidence of residual tumor. The IoMRI scan served as the
early postoperative MRI if the IoMRI revealed complete tumor
resection or satisfactory degree of subtotal/near-total resection.
Repeat IoMRI was performed if further tumor resection was performed
after the first IoMRI. Contrast agent was used during IoMRI if the tumors demonstrated enhancement
on preoperative imaging. The majority of the children received only
one dose of contrast during the first and only IoMRI study. The
duration of the IoMRI varied between 10-60 min according to the
required studies to
update a complete early intraoperative
study or studies.
The IoMRI interpretation was performed by the operating neurosurgeon. If the IoMRI findings
led to further tumor resection, tissue samples were obtained for
histopathologic analysis.
Following the IoMRI, the patient is transferred back to the
operating theater, where the images are immediately available to the
neurosurgeon using advanced multimodal image display technology.
Among the MRI neuro clinical applications,
MRI spectroscopy 15 is the most important one in presence of brain
masses. It can with confidence tell if the lesion is an abscess,
lymphoma, active multiple sclerosis lesion, grade of malignancy of
the brain tumors.12 It is useful tool before surgery,
that when the patient coming with report as having brain tumor, to
end with an abscess. It is useful even during surgery to
differentiate the tumor residual from hematoma due to surgical
intervention. Even with strict hemostasis, when you send the patient
to the MRI some amount of hematoma accumulate, and SWI and
spectroscopy can help in the nature of the residual.
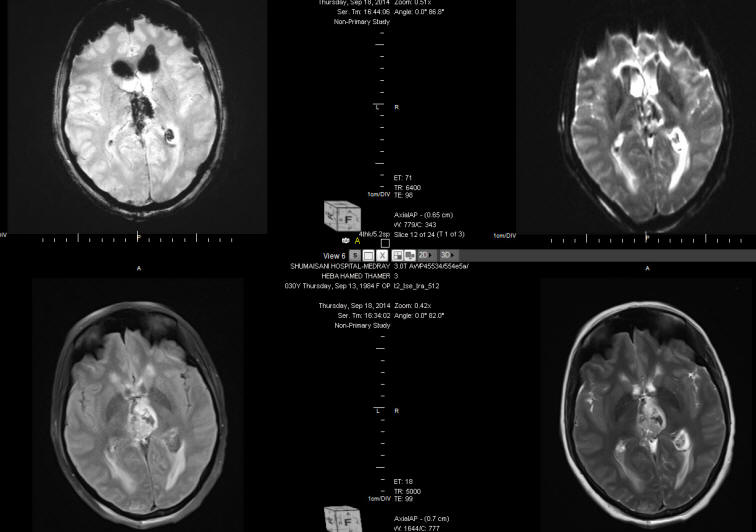
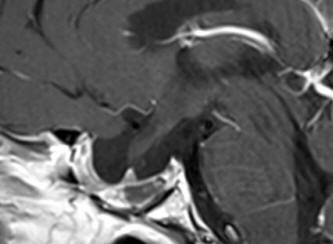
Below, showing a case with posterior third
ventricular anaplastic ganglioma in 30 years old patient to whom
intraoperative MRI with spectroscopy, SWI and MRA were performed
twice to confirm the total resection of the tumor. See fig-1-7.
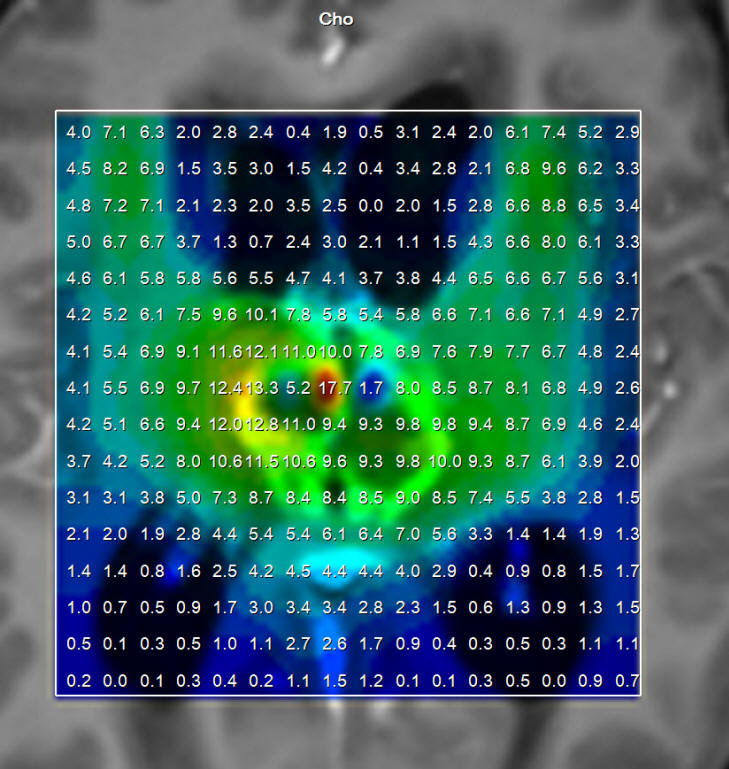
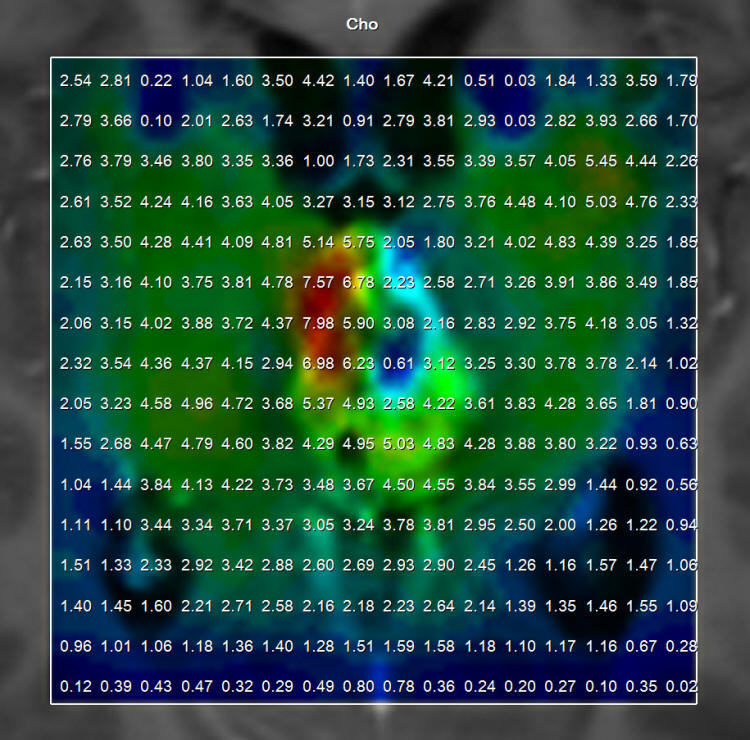
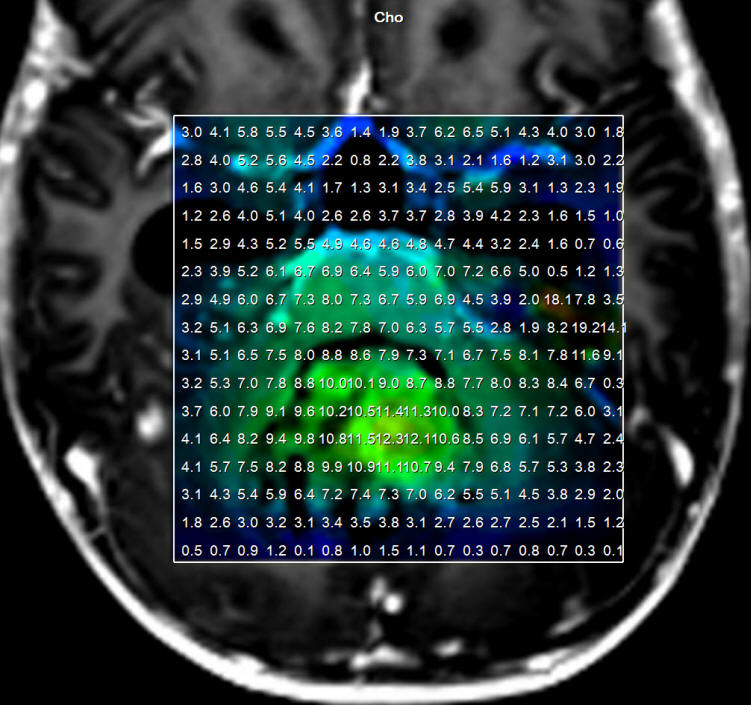
Fig-1:
Choline distribution showing a small nidus of possible malignant
character befor attacking the lesion.
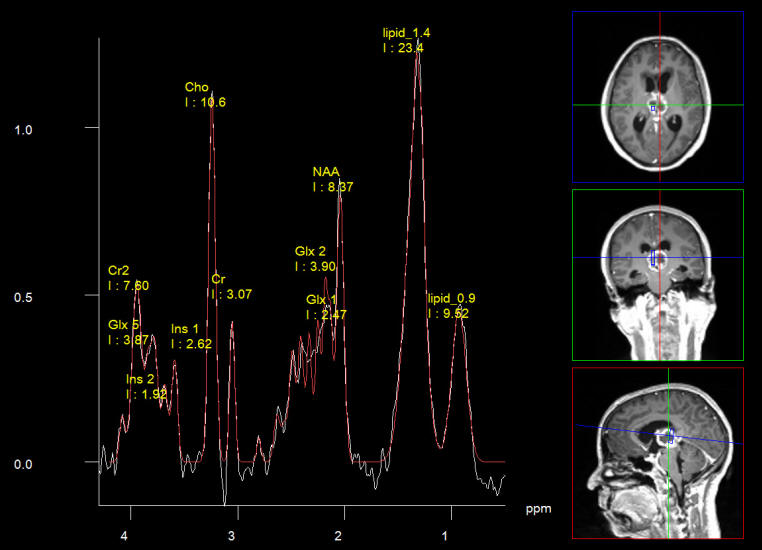
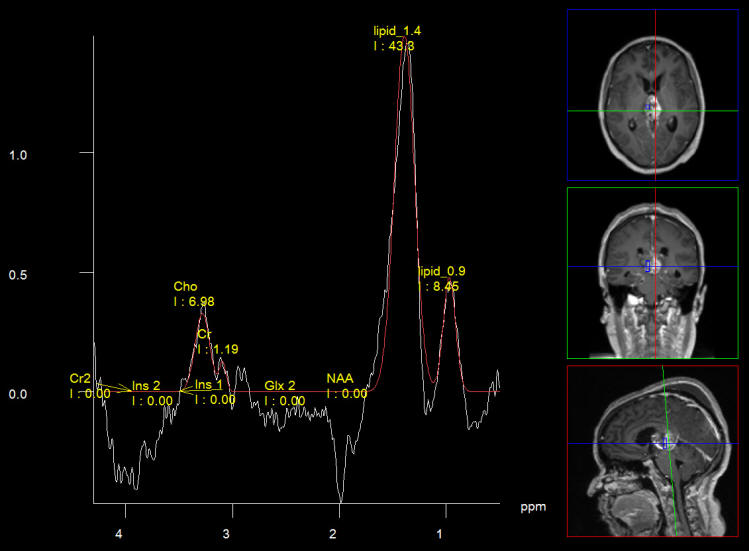
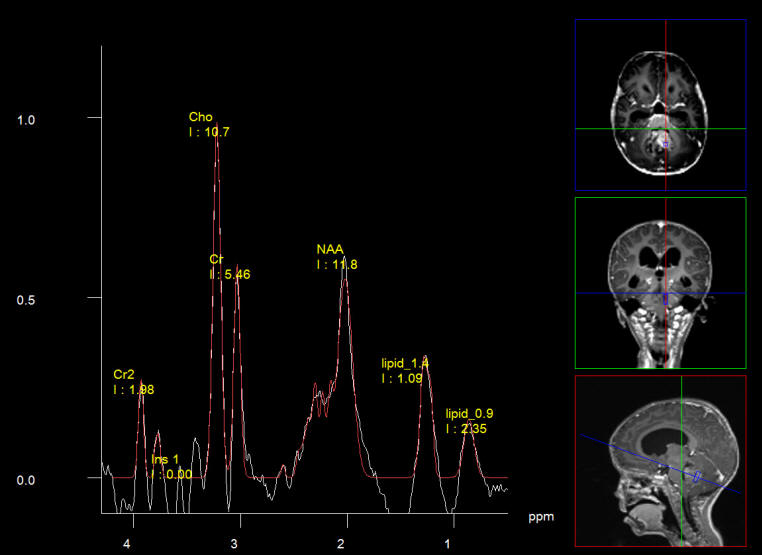
Fig-2:
Short Echo spectroscopy in favor of pinealoblastoma, which proved
later to be anaplastic ganglioglioma. These data before attacking
the lesion.
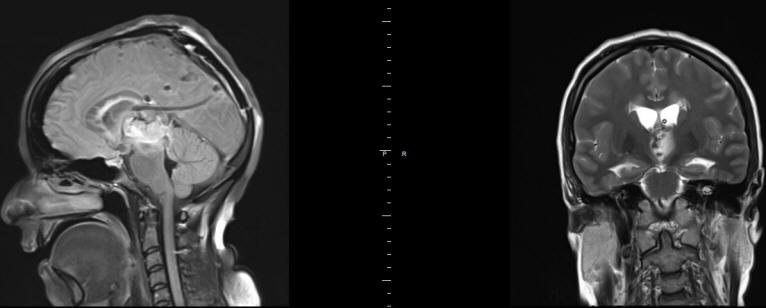
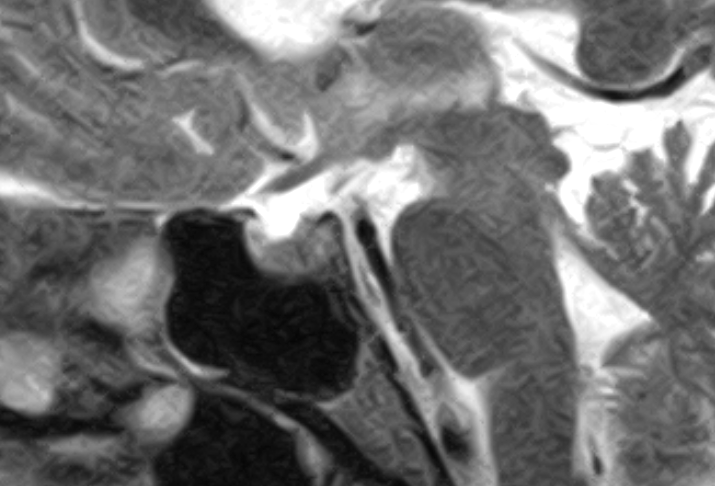
Fig-3:
The next intraoperative MRI showing total resection of the mass and
floating venous structures with deformed choroidal veins.
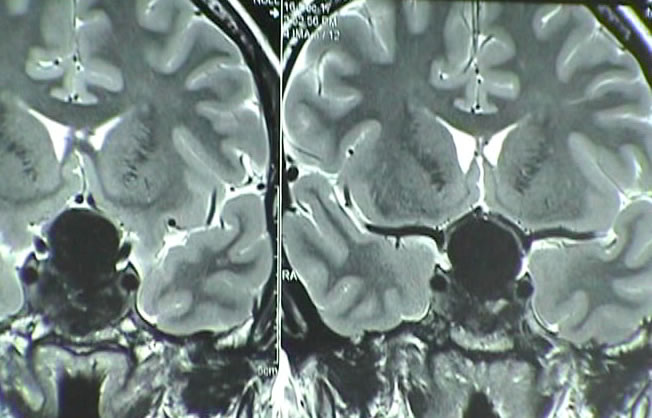
Fig-4:
Saggital and coronal views showing the external drain and
a clot over the mesencephalon.
Fig-5:
Choline elevation confirming still persisting active sites
intermingled with the hematoma in the right side.
Fig-6:
Spectroscopy short TE showing low choline ratio? with high lipids
1.3 and 0.9. confirming resection of the residual
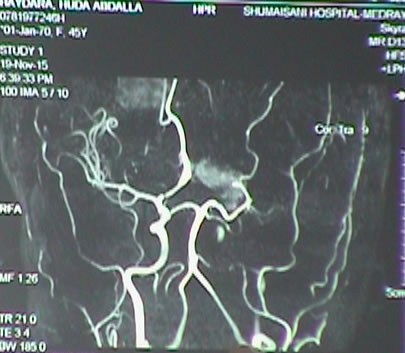
Fig-7:
The hematoma in the bed of resected tumor. Notice that there is no
arterial spasm.
The patient had smooth
postoperative recovery, but later progressed transitory mutis after
tapering Decadron, which resolved over 2 weeks. The challenge in
this case was to preserve all the running veins in this area.
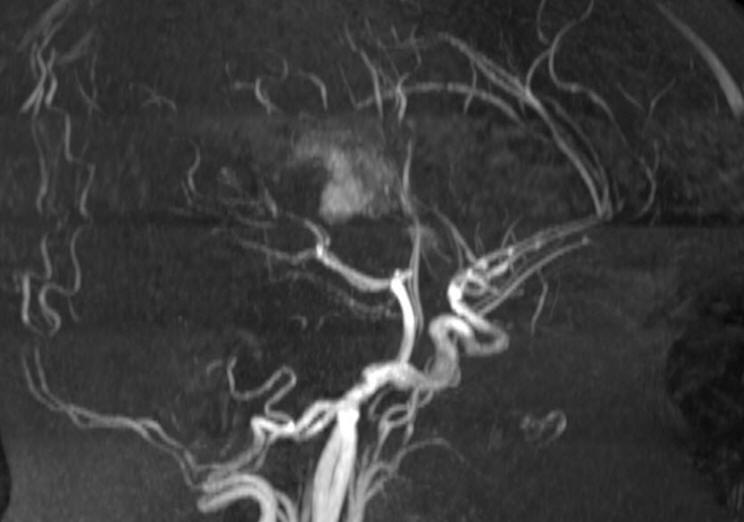
In another case with patient operated by me
14-November-2006 for huge craniopharyngioma through subfrontal
approach with mobilization and preservation of the olfactory tracts.
The patient then developed recurrence and was operated by me
26-May-2015. During the second surgery an Ommaya reservoir must be
directed from a point without violating the vascular structures and
the CSF to avoid contamination. The following figures (8-13) showing
the case:
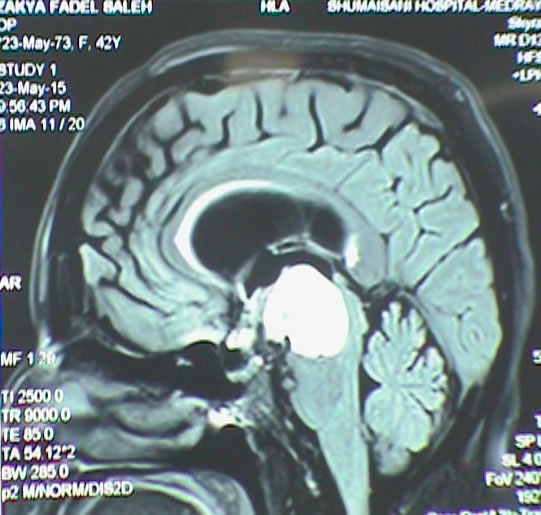
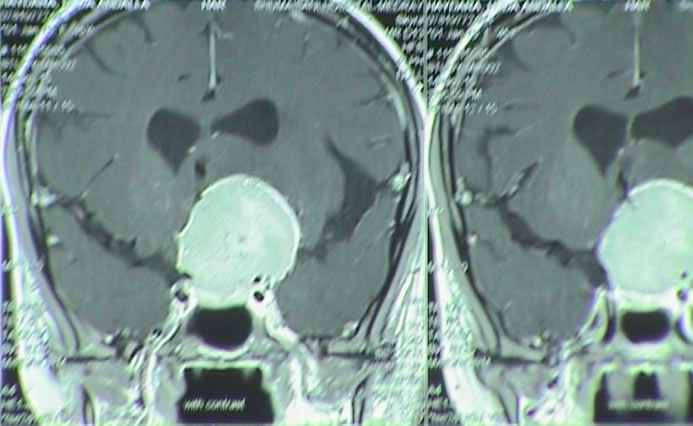
Fig-8: MRI showing the cystic craniopharyngeal
cyst pushing the mesencephalon inferior.
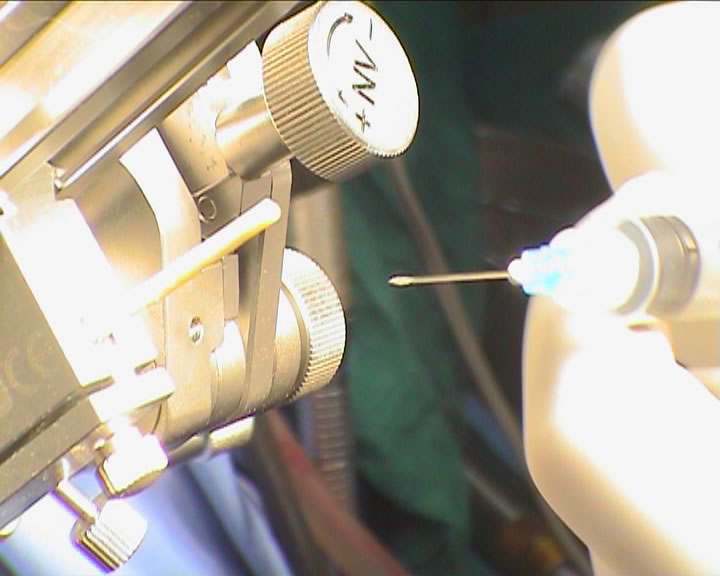
Fig-9: The ceramic ring fixed with localizer
and sent to MRI with TxRx head coil to perform coordinated data to
the iPs 5 planning software.
Fig-10: The trajectory was exactly planned to
have the tube in the most dependant point of the cyst without
contaminating the CSF.
Fig-11: Evacuation of the yellow-brown
craniopharyngeal cystic component.
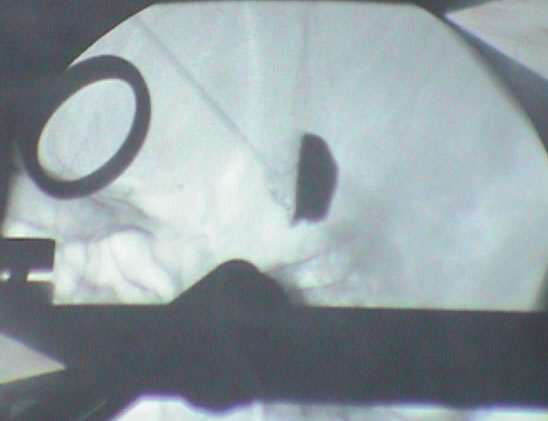
Fig-12: Contrast material injected to the
cavity to be visible in the C-arm.
Fig-13: Contrast material removed from the
cavity to be visible in the C-arm.
The patient was discharged the next day and
followed for several years.
The following case demonstrating the role of IoMRI
and Io neurophysiologic control and application of bipolar pulsed
mode radiofrequency in spine surgery:
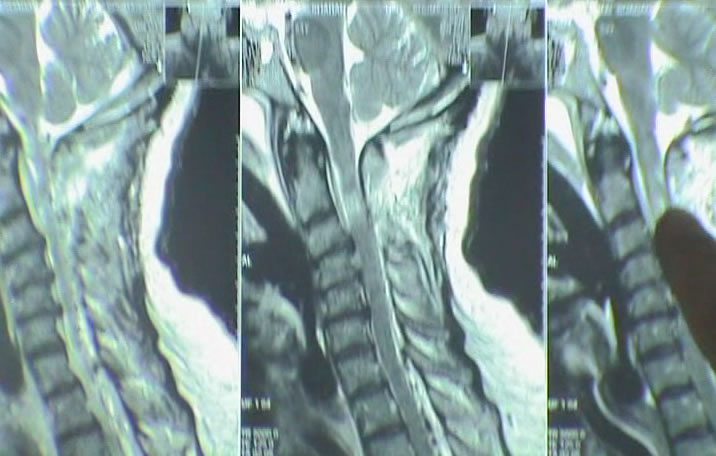
The patient a female 53 years came to the clinic 03-September-2016
complaining of neck and right upper limb pain for 4 years with
progressing numbness right hand. MRI cervical spine spine performed
01-September-2016 without report and very bad quality, showing as be
an intramedullary mass behind C1-2-3.
On examination, the patient had no pain when turning the head to all
direction. There was weak right deltoid 3/5, left 4/5, right biceps
-4/5, left 4/5, flexion right hand 3/5, left 4/5, extension right
hand -3/5, left 3/5, right triceps 4/5, left 5/5. There was weak
dorsiflexion right foot -4/5, left 4/5. The deep reflexes were
exaggerated in the right side, but no pathologic reflexes. There was
no apparent sensory deficit.
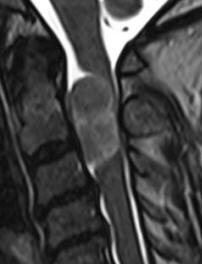
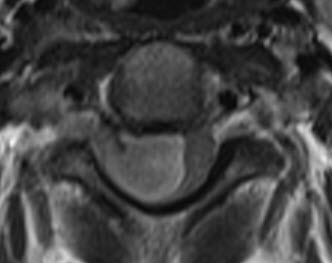
The patient was sent for thorough investigations and MRI cervical
spine performed 04-September-2016 showed huge meningioma 33x12.7 mm
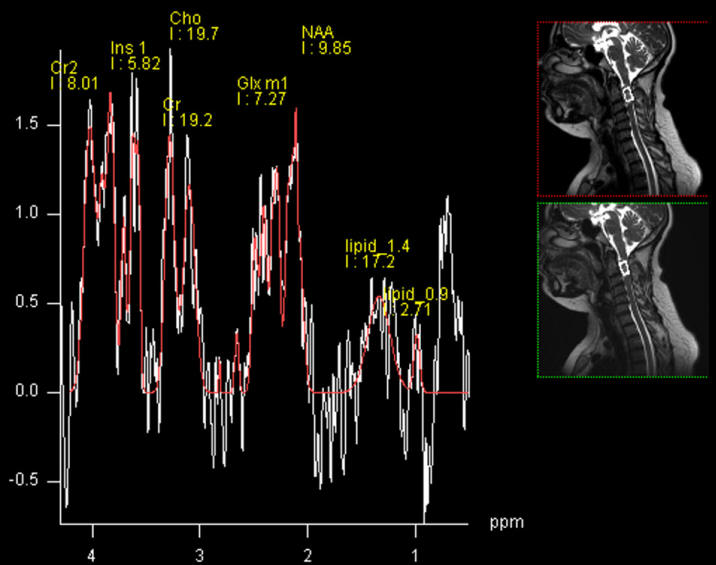
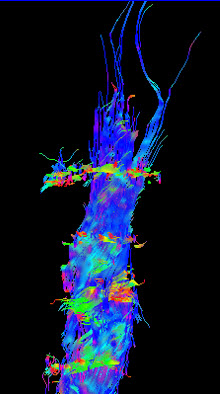
intradurally pushing the spinal cord to the left. Spectroscopy was
typical for meningioma and the mass was lacking fibers. There was
and extension to the right C1-2 foramen reaching the vertebral
artery pushing it anterior.
In prone position with the use of IOM ISIS, laminectomy of C2-3 and
partial of C1 was achieved. The dura was opened slightly right
parallel to the midline. The dumbbell-shaped appearance of the tumor
was due to right C2 anterior and posterior rootlets, which were
constricting the tumor and they were preserved to the end of
surgery. The matrix of the meningioma was the right lateral wall of
the dura, which was coagulated and piece-meal resection of the tumor
was performed. MEP was troubleshooting and not informative. After
the resection of the tumor a tiny piece and the emergence of the
right C1 was removed trying during that to preserve the rootlets.
Using MultiGen, bipolar motor stimulation of right C2 was achieved
with 1.0 V. Motor stimulation of the right side of the spinal cord
and a brisk response of the right upper and lower limbs was achieved
above the tumor resection area. Irrigation of the area with 1
ampoule Papaverine diluted with 20 ml saline. The dura was closed
water-tightly. Routine closure of the wound. The patient was sent to
MRI before extubation.
Smooth postoperative recovery. She showed deep paralysis of the
right upper and lower limbs, which started to improve over several
hours. She was sent to the ICU. Figures (14-21) demonstrating the
case.
Fig-14:
The meningioma in different sections and sequences.
Fig-15:
Single voxel Spectroscopy showing the peak at 3.8 ppm characteristic
for meningiomas. For more information,
click
here!
Fig-16: Absence of fibers confirming nonglial nature of the
mass.
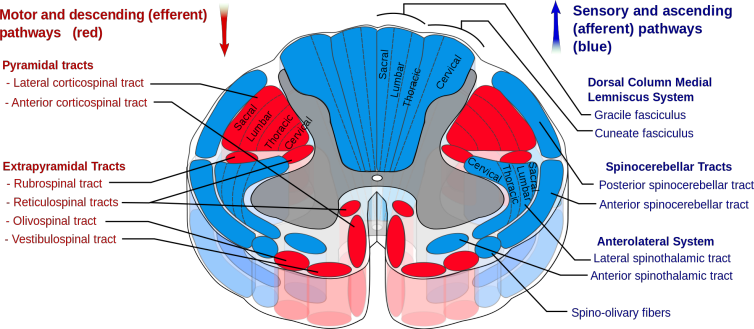
Fig-17:
Anatomical architecture of the spinal cord at C2-C3 level.
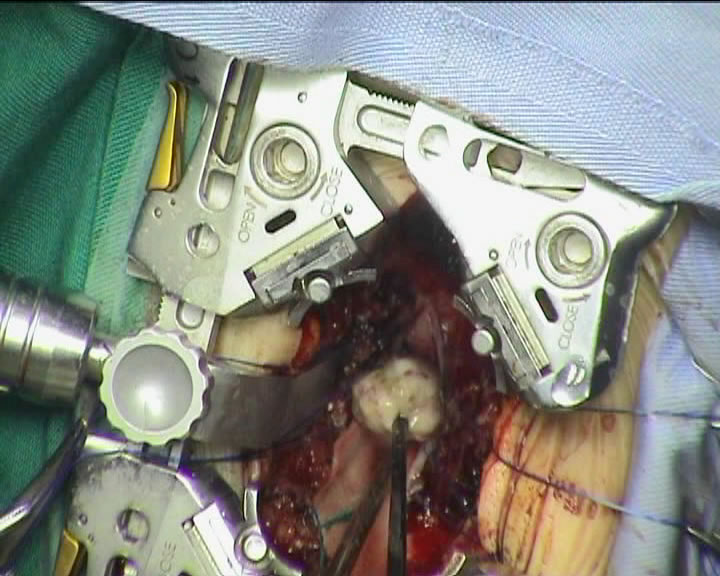
Fig-18: Resection of the last piece.
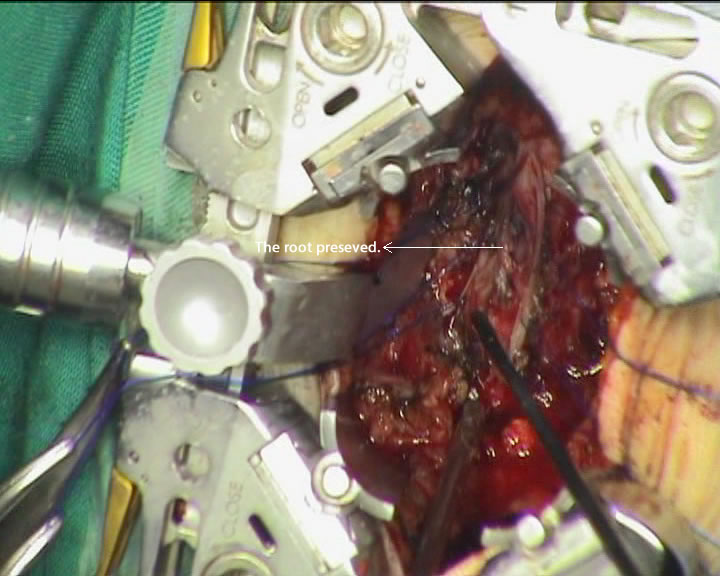
Fig-19: The meningioma totally resected with
preservation of the crossing root.
Fig-20: Check MRI before extubation.
Fig-21: Check MRI before extubation,
Follow Up
The patient came 03-October-2016 to the clinic walking without aid:
The motor function normalized and having numbness left side of the
body. The postoperative recovery was amazingly excellent. The wound
was clean and she suffered from occipital headache with neck pain.
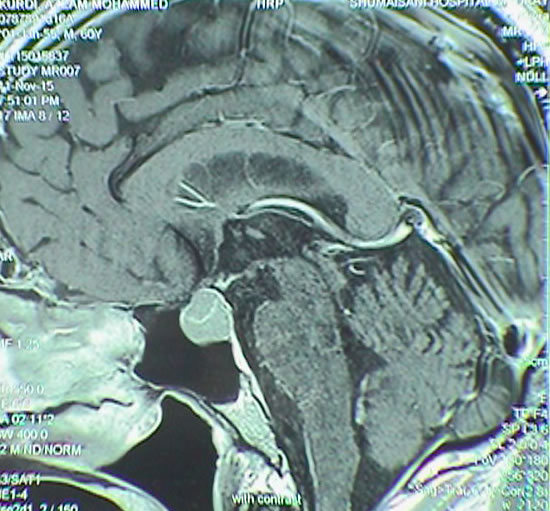
The following case demonstrate the radical
resection of pituitary adenoma even with transphenoidal approach: The
patient is a doctor of psychiatry 60 years old came 11-November-2015
complaining of general weakness and fainting attacks for 4 years and
diagnosed as having prolactinoma. He is diabetic for 10 years with
hypertension for 20 years. Signs of panhypoptuitarism were found and
treated with L-thyroxin, testosterone and Dystinox 1/2 tab every 2
days. MRI sella done 29-December-2013 and repeated 14-October-2015
showing the macroadenoma is progressing in size and start to
compress the optic chiasm from the left and right parasellar
extension. The patient noticed visual disturbances of the left eye
the last 3 months. PRL level was 6.3 µIU/ml performed
14-October-2015.
The patient was sent for investigations and MRI done
11-November-2015 showing the pituitary adenoma and the MRA showed
the relation of the vascular relation to the mass.
Transphenoidal approach guided with the C-arm until the anterior
wall of the sphenoid sinus reached through the right nostril. The
floor of the sella turcica was partially removed to reach the tumor.
The tumor is soft in consistency and it was sent for histologic
verification. The tumor was removed trying to preserve the pituitary
gland, which is actually the tumor capsule. The eroded dorsum sella
was seen. A cavity was obtained inside to pituitary gland. MRI
control showed remnant of the tumor at the left side. This part was
removed and further removal of the tumor was obtained. 2 Eonmedltech
nasal packs with tubes were inserted and another control MRI was
performed. The almost radically removed, but packs are directed
toward the tumor. They were removed and reinserted to the pharyngio-nasal
cavity. The patient then was extubated.
Smooth postoperative recovery. The patient was sent to the ward.
Fig-22: The macroadenoma before surgery.
Fig-23: Intraoperative MRI confirming still
having the tumor.
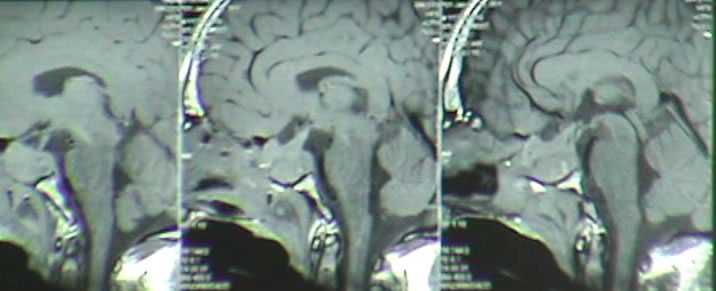
Fig: 24 Control MRI of the sella performed
23-December-2015 demonstrating radical resection of the pituitary adenoma. Frontal view.
Fig-25:
Saggital view.
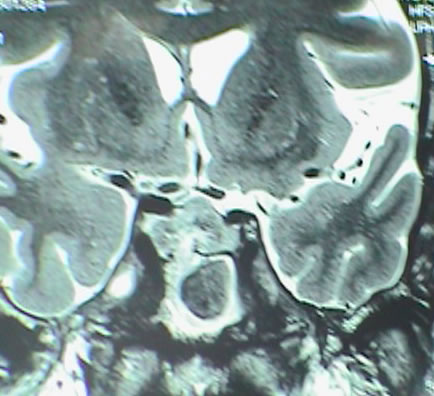
Another case with massive suprasellar extension: The patient came 36
years old to the clinic 14-December-2017 complaining of blurred
vision left eye for three years. The last week go almost blind left
eye with decreased vision right eye. MRI done in Turkey
11-December-2017 showing huge pituitary adenoma with massive
infrasellar and moderate suprasellar extension with signs of
apoplexy of the tumor bed with fluid level inside the tumor. The
patient is convulsion free.
On examination, the patient can feel the light in the left eye and
can count the fingers around 1 meter before the right eye. The
oculo-motor innervation is intact. There is no galactorrhea.
Normosmia. There are manifestations of panhypoptuitarism, but no
data for diabetes insipidus.
The patient was sent for thorough radio-ophthalmo-endocrine
investigations. MRI of the sella with MRA done 16-December-2017
showed the tumor pushing the chiasm and optic nerves with
suprasellar extension around 16.2 mm. The tumor has massive
infrasellar extension reaching the naso-pharyngeal space abutting
it. The tumor dimensions are 37.3x28.6 mm. There is no invasion of
the cavernous sinuses. There is fluid level inside the tumor
confirming the presence of apoplexy. Visual acuity of the right eye
after correction 6/6. The left eye 6/0.05. There is massive scatoma
left eye with less in the right eye. Prolactine 470 ng/ml, LH 1.19,
testosterone 0.3. Considering the above data trans-sphenoidal
approach with MRI control was advised. Mathematically speaking the
volume of the tumor with the hypophysis is around 8.8 ml.
Fig-26:- Preoperative MRI Showing the huge
suprasellar extension.
Fig-27: Preoperative MRI Saggital view.
The patient was put in setting position to
perform trans-sphenoidal approach with the C-arm projecting to the
sella turcica. A trial to evacuate the tumor by epidural needle 14
was attempted and brownish content was achieved.
Fig-28: Attempt to evacuate the tumor by
syringe failed and checked by MRI showing mild reduction.
Fig-29: The tumor resected. Notice the swollen
pituitary stalk .
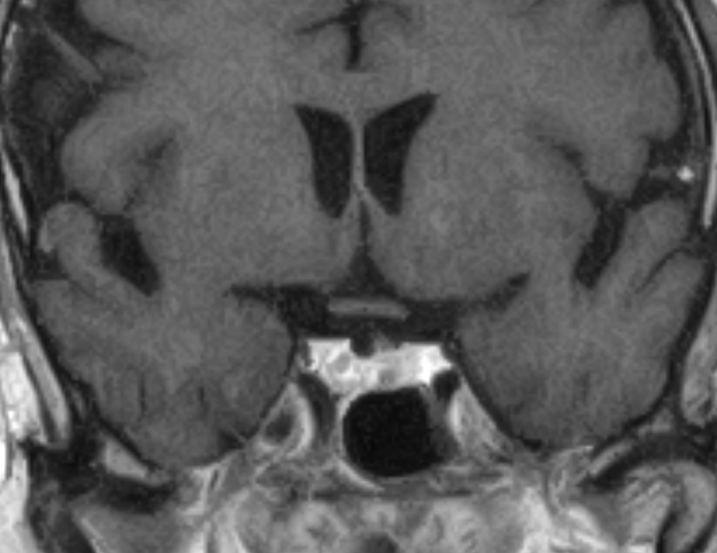
The patient was sent for MRI control. The
tumor still there with new bleeding inside the evacuated cavity. The
puncture site was extended and the rubbery pituitary inferior wall
was incised. The tumor was removed using curettes for biopsy and the
remaining was removed by suction. It was possible to see the
posterior borders of the pituitary gland. Using Omnipaque diluted
3cc was injected to the tumor cavity. It is pulsating well,
manifesting the absence of suprasellar part of the tumor. The
patient was sent another time for MRI control. The tumor practically
resected with the pituitary stalk hanging free and the optic nerves
more than 8 mm above the superior surface of the preserved pituitary
gland. There is no bleeding inside the cavity. Routine closure with
tampons of nostrils.
Smooth postoperative recovery. The patient was sent to the ward.
Follow up MRIs after several months showed disappearance of the
edema of the stalk and shrinkage of the swollen pituitary
gland.
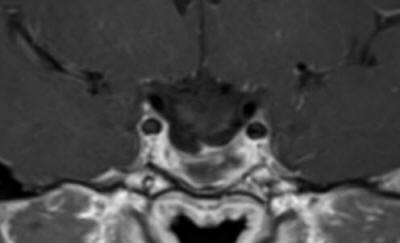
Fig-30: The sellar content 3 months after completion of
radiotherapy. MRI performed 14-January-2019.
Several Authors now performing transphenoidal pituitary
adenoma resection with IoMRI.14
I n another case with medulloblastoma: The
patient 4 years age came to the clinic with his parents
27-January-2015 complaining of vomiting and drowsiness for 1 month
with the last weak complaining of diffuse headache. CT-scan done
25-January-2015, showing a midline posterior fossa mass.
On examination, Considering his age, it was difficult to evaluate
him for Romberg positioning, but there was no nystagmus and
neurologically was free.
The patient was admitted urgently to the hospital and MRI of the
brain with contrast with MRA of the brain and carotids with
spectroscopy and DTI were performed under G.A. There is huge
medulloblastoma vermian localization with extension to both foramina
of Leuschko. So as to avoid putting shunt to him, massive doses of
Decadron were started and the patient started to improve.
Fig: 31:-
Spectroscopy showing typical data for medulloblastoma
Fig-32: Choline distribution in the medulloblastoma.
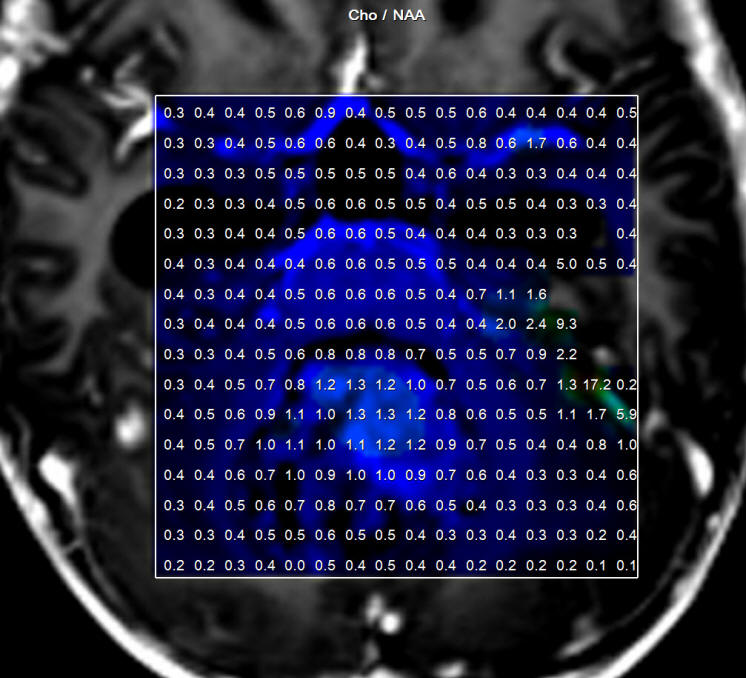
Fig-33:
Cho/NAA ration distribution of the medulloblastoma.
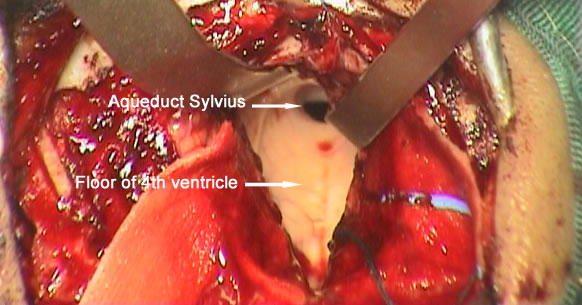
Fig-34:
Floor of the 4th ventricle after removal of the medulloblastoma.
Midline posterior occipital approach in
setting position. The bone flap reflected to the neck inferior. The
dura was opened in V-shape fashion. The tonsils were shifted
downward and the vermis is prominent by the tumor. Sharp dissection
of the inferior pole of the vermis ( The uvula). The tumor was
highly vascular with rich blood supply. The tumor was coagulated
sucked and most of the upper part was removed. The inferior part was
was removed until the obex with related structures were seen. The
left part of the tumor was followed and resected until the foramen
of Leuschko was seen and the left inferior cerebellar peduncle was
preserved. The same maneuver was undertaken in the right side. The
tumor inside the 4th ventricle was removed and the floor of the 4th
ventricle was seen intact with widened aqueduct through which the
third ventricle was seen. The superior medullary velum was
respected. The floor of the 4th ventricle was flattened due to the
previous compression effect of the tumor, that it was impossible to
see the median sulcus, nor the paramedian sulci limitantes or the
hypoglossal trigone elevations at the calamis scriptorius. I got the
impression that the tumor was totally resected, for what
intraoperative MRI control with contrast was done.
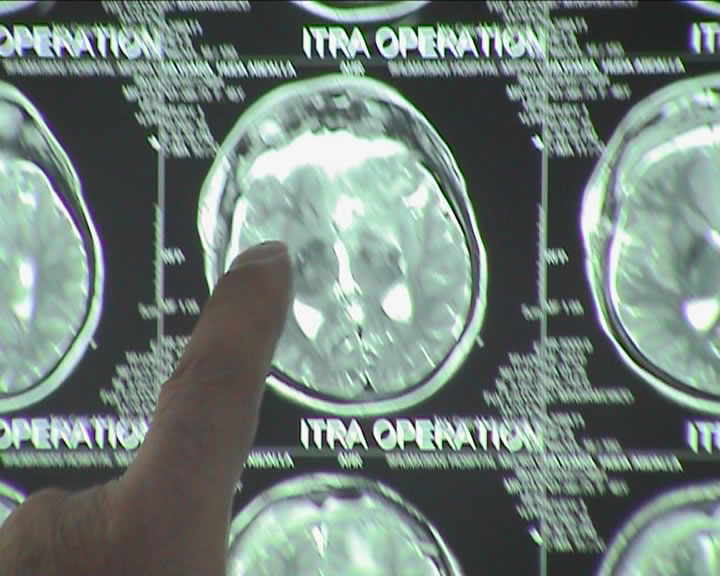
Fig-35: transfer to MRI for first check up.
Fig-36:
MRI done during surgery showing the missing part of the tumor, which
was subsequently removed.
There is still part of the tumor in the right
upper corner and the right foramen of Leuschko. Resection of this
part was achieved until the normal cerebellar tissues were seen at
these angles. Strict hemostasis with water-tight closure of the dura
and bone flap was secured with 2 stitches and routine closure of the
wound.
Smooth postoperative recovery. The patient extubated and sent to the
ICU for 24 hours observation.
The patient has typical spectroscopic data supporting
medulloblastoma. The histologic result was medulloblastoma.
Despite the availability of all these
technologies, complications can be recorded intraoperatively in MRI
and some of them are fatal as in this case:
The patient a lady came to the clinic 14-November-2015 complaining
of blind left eye for 3 years with bifrontal headache for 2 years
and almost blind right eye for 8 months. On examination; the patient
is blind in the left eye and can differentiate fingers 10 cm near
the right eye. The right eye shift lateral when looking anterior
with horizontal nystagmus when looking to the right.
The patient was sent for investigations and MRI done
14-November-2015 showing a giant meningioma involving the planum
sphenoidale and tuberculum sella with massive supra-retrosellar
growth more to the left with left optic nerve canal extension and
stretching with spasm of the left A1 and edema of the left frontal
lobe.
Bifrontal craniotomy with reflection of the bone flap to the right.
The frontal sinuses were violated and the mucosa stripped
accordingly. The dura was opened parallel to the base of the
anterior fossa and both olfactory tracts were dissected off the
mediobasl frontal lobes, but the left one was completely destroyed
by the tumor and it was not possible to dissect it to the trigone
for what it was intentionally bisected to remove the anterior part
of the tumor. The tumor was rich in feeders and it was necessary to
remove it by piece-meal fashion after coagulation. That part
compressing the right optic nerve was removed, but at the junction
with the chiasm, the tumor was stuck with optic nerve, for what a
tiny layer was lift intentionally to preserve the right optic nerve.
That part which was extending to the left optic canal was removed,
but a thin layer stuck with left ICA was left to avoid vasospasm. It
was coagulated. The tumor was followed posteriorly until the basilar
artery was seen with Liliquest membrane has defect due to tumor
invasion. Most of the time dissection was carried at the area of the
right A1 segment and the tumor was maximally removed. It was
possible to expose the chiasm at its medial part, which was pushed
posterior. The area of the left A1 segment was not violated and to
avoid possible bleeding from this segment, a Surgicele was applied
to this area. All the feeders which were many, were coagulated and
bisected by microscissors. Strict hemostasis and routine closure of
the wound with repair of the frontal sinuses by muscle harvested
from the left thigh. The patient was sent MRI to investigate the
circulation, since a lot of vascular dissection was carried out,
especially the right side. MRI showed severe spasm of the left ICA
at the bifurcation from the left CCA. MRI with contrast showed
branched of the left M1 and the left A1. This could be due to
transitory spasm. All measure were to taken to resolve the spasm.16
They failed. The patient then was extubated. Figures (22-26).
Smooth postoperative recovery. The patient showed at the start right
side paresis, which resolved over minutes. She was sent to the ICU
for 24 hour observation.
The patient progressed right sided paresis with pronounced
spasticity 2 hours after surgery. The next day the right limbs
improved and the spasticity gone, but she developed diabetes
insipidus for what Minirin was started. She still have total
aphasia.
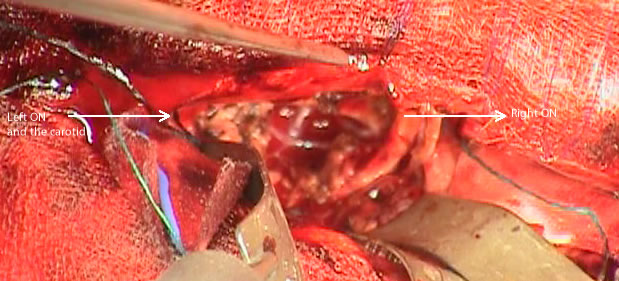
Fig-37: The tumor before surgery.
Fig-38: Surgical field after resection. Notice
the left ICA looking normal and the right olfactory tract preserved.
Fig-39: Transferring the patient to MRI, before extubation.
Fig-40: Complete resection achieved.
Fig-41: The patient showing arterial spasm of the left ICA in the
neck.
The patient died the 5th postoperative day
despite all measures to fight with the arterial spasm and removal of
the bone flap performed 3 days after the first surgery. This case
showed that despite using all these techniques, some problems
remain and will still unable to resolve them, even when you see them
in real time
and try your best.
Our initial results have been encouraging and further research is
required to evaluate the clinical effectiveness of IoMRI in the
management of specific tumors and the role of advanced MRI
techniques in the intraoperative context.
The ceiling
suspended and the MRI moving to the operating room were omitted from
our plan, because of the fear of troubleshooting the constructs.
Instead we purchased the another dockable table to be ready to
replace the first in case of troubleshooting.
RESULTS
IoMRI was used during 20 cranial mass resections in 15 adults and 5 children.
Overall, IoMRI scan led to further surgery in all these cases.
Complete surgical resection was
intended in (80%) operations. IoMRI findings suggested
complete resection in (40%), residual disease in (20%),
and equivocal residual disease in (10%) patients. All cases were
apparent tumor free after first or second intraoperative MRI check
up. Follow-up MRI scans at 3 months in 6/7
patients with equivocal IoMRI did not show any evidence of residual
tumor, and therefore these patients could be classified as complete
tumor resection, making the total number in this category as (80%).
DISCUSSION
Intraoperative MRI having place in practice for 20 years and it took
several trails and versions to accomplish.[7]
IoMRI has become increasingly important as a tool to aid safe and
complete resection of brain tumors in adults, and is expected to
make a major contribution to neurosurgery for pediatric brain
tumors. In a study of adults with low-grade gliomas, Pamir et al.
have reported that 3-T IoMRI led to further resection in up to 40%
of cases and increased the proportion of complete tumor resections
by over 30%.[8] In another study of adult patients with high-grade
gliomas, the use of a low-field IoMRI increased the proportion of
complete macroscopic tumor resection from 36 to 75%.[4]
Computer-assisted neuronavigation using preoperative MRI is now
considered standard care and has facilitated radical tumor resection
and increased survival in adults. In a study of 104 adults with
glioblastoma treated surgically, the use of image-guided
neuronavigation led to complete macroscopic tumor resection in 31%
using neuronavigation, but only 19% without neuronavigation. The use
of neuronavigation and complete tumor resection were associated with
a highly significant increase in patient survival.[10]
Other than high-field MRI, other modalities for intraoperative brain
imaging include ultrasound (US), computed tomography (CT; using
either fixed or mobile scanners), and low- and medium-field MRI.
It is
important to note that none of these alternative intraoperative
modalities can match the diagnostic accuracy of high-field MRI in
the evaluation and documentation of completeness of tumor resection
now required for modern treatment protocols. In addition, IoMRI can
obviate the need for postoperative MRI imaging which will otherwise
be needed within 24 h of surgery to document the extent of tumor
excision. This is particularly useful if the child is in an unstable
clinical condition in the postoperative period and in children who
would otherwise require a second general anesthetic for postoperative
high-field MRI scan to document the extent of tumor excision.
The extent of resection is an important predictor of prognosis in
children with medulloblastoma, ependymoma, and high-grade
glioma.[1,9,11] Traditionally, this has led to reoperation following
early postsurgical scan. IoMRI now provides the opportunity to
identify cases where the surgical aim has not been met and extended
resection is possible. In our initial experience, IoMRI has resulted
in extended surgical resection in all operations, including
26% where complete resection was intended and 41% where partial
resection was intended. In literature, the reported rates
of extended resection vary between 27.5 and 60%. Our results are
similar to those reported by Nimsky et al.[6] in their initial
experience with 1.5-T IoMRI, where the surgical strategy was
modified in 27.5% of the first 200 patients (both children and
adults). In a recent paper, Levy et al. have reported their
experience in 98 children who underwent IoMRI using a 1.5-T scanner.
In this study, 25 adults and children underwent surgery for brain tumors, and
in 60% of these, IoMRI led to further surgery.[5] Variations in the
rate of extended resection are likely to occur given the diverse
patient groups, tumor types, and surgical and radiological
expertise. On balance, the results to date, indicate
that IoMRI has led to improved tumor resection and further research
is required to assess the clinical outcome for individual patient
groups.
In our experience, high-field IoMRI has not only improved the
percentage of gross total resection in keeping with the surgical
goal, but also proven invaluable in the surgical management of
deep-seated tumors in eloquent areas where the surgical goal had
been limited resection. In 20% of our patients where the surgical
goal was subtotal resection, further resection was carried out
following IoMRI. This is particularly relevant in surgical
management of deep-seated chiasmatic/hypothalamic gliomas where a
midline approach (transcallosal interforniceal) gives a minimally
invasive but limited view of often very large tumors. In these
cases, a planned IoMRI at the halfway stage to evaluate progress and
fine-tune the final resection has been very useful. IoMRI adds
safety to this type of surgery and allows the surgeon to make an
informed decision about the amount of residual tumor to be left,
while minimizing the damage to functionally important structures
such as the hypothalamus and optic chiasm. Another application of
IoMRI is to confirm the biopsy tract and that representative tumor
areas have been biopsied.
IoMRI has not only reduced the need for early reoperation, but also
reduced the number of early postoperative MRI scans, previously
performed routinely between 24 and 48 h post surgery. In our
practice, the final IoMRI scan has replaced the postoperative MRI
scan and helped to streamline patient care pathway.
Evaluation of IoMRI studies pose certain challenges, and although we
have not encountered significant problems with interpretation of
IoMRI, they are well described in literature. These include
susceptibility artifacts, surgically induced contrast enhancement,
and brain shift.
Susceptibility artifact can occur from external sources including
metallic objects (even if nominally MRI compatible) such as head
holder pins and endotracheal tubes or intracranial sources including
hemorrhage and air introduced during surgery. Gradient- and echo
planar-sequences are the most affected. The use of titanium pins to
hold the head minimizes susceptibility artifact. Also, the pins are
usually placed away from the region of interest to minimize the
influence of susceptibility artifact on image interpretation.
We use MRI compatible endotracheal tubes and carbonized pins, which
are free of artifacts. Placing the cuff of the endotracheal tube on the chest rather than
beside the head can reduce the associated artifact. Irrigation of
surgical cavity reduces the amount of intracranial and intracavitary
air.
Surgically induced contrast enhancement is a potential cause for
misinterpretation during brain tumor resection. The following four
types of contrast enhancement induced by surgery have been
described:[3]
1.
meningeal enhancement,
2. Increased enhancement of the choroid plexus,
3. Delayed enhancement of the surgical margin, and
4. Immediate intraparenchymal enhancement.
The latter two are thought to be caused by leakage of contrast
material from surgically open vessels or transient blood brain
barrier disruption and have a greater potential to be misinterpreted
as residual tumor. This phenomenon is particularly important in
tumors with cystic components and at a site where a bipolar
cauterizing instrument has been used during surgery. Careful
comparison with preoperative imaging is advisable in these
circumstances.
Intraoperative brain tissue deformation (brain shift) is frequently multifactorial. These include
reduction in tumor mass, collapse of the resection cavity, edema,
hemorrhage, and drainage of cerebrospinal fluid. Careful comparison
of anatomical landmarks including the sulci, the gyri, the vessels,
and the non-deformed parenchymal structures is useful in
orientation. Diffusion tensor imaging with fiber tracking may be
helpful in this situation.
CONCLUSION
In our experience, when managing all neurosurgical and spine cases, the IoMRI
aided with all neuro software, provides us
with the ability to illustrate, document, and discuss all aspects of
surgery and is a significant improvement in the quality of patient
care. Being able to confirm the achievement of surgical aims
immediately before extubating the patient and even to
decide, who can awakened, or to keep him in ventilator,
is an immeasurable quality leap in parent
satisfaction and experience. This technology has transformed our
management approach to brain tumor in all patients by influencing
surgical decisions and increasing the rate of complete tumor
resection and the extent of partial tumor resection. Optimal use of
this expensive intraoperative facility requires careful planning and
management. Equivocal findings resulting from postsurgical contrast
enhancement can pose challenges. When you merge the data obtained
from neurophysiologic intraoperative monitoring, such as MEP, SEP,
VEP, AEP, EEG, EMG, PRESP and you have a lot of data, enforcing to
have a new look to phenomena such as transitory postoperative
paraplegia, when the neural structures having a good look after
tumor resection. Further studies involving larger
numbers of patients/procedures, outcome, and the use of advanced
IoMRI techniques need to be encouraged.
Footnotes
Disclaimer: The author of this paper have received no outside
funding, and have nothing to disclose.
Skyra MRI with all clinical applications in the run since 28-Novemeber-2013.
Inomed Riechert-Mundinger System, with three point
fixation is the most accurate system in the market. The microdrive and
its sensor gives feed
MER Inomed system.
Inomed ISIS IOM
highline with 32 channel and Neuroexplorer version 5 is functioning for
several months, starting from 01-August-2007. For more detailed information
about this functional neuronavigation machine with its early alarming signals,
please refer to inomed.com
Leica HM500
The World's first and the only Head mounted Microscope.
Freedom combined with Outstanding Vision, but very bad video recording and
documentation.
After long years TRUMPF TruSystem 7500 is running with in the neurosuite at
Shmaisani hospital starting from 23-March-2014